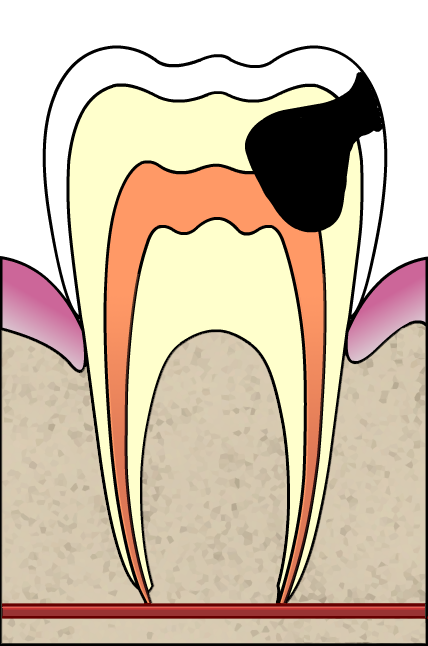
Pulp capping is derived from the name pulp cap which means trying to sterilize the damaged tooth area as well as one can, followed by stopping the bleeding and placing the right filling material on it. The precaution being that teeth that are already abscessed should never be pulp-capped – this is done to those teeth where the nerve is irritated but still alive and healthy enough to repair the self given a chance to do so. Pulp capping gives it a chance by getting out the decayed portions and the bacteria then putting a clean dressing on it with the filling
After eliminating the wounded dental tissues of a carious tooth, the next step is usually filing the cavity with a suitable restoring material. When pulpal tissue is exposed it gets contaminated by bacteria and mostly these are the conditions that warrant the clinician to perform pulp capping. When performing this procedure, the degree of the pain and the pulpal size exposure are considered.

This procedure was traditionally carried out using calcium hydroxide formulations that have bactericidal effects; it has been shown that this dentinal bridge is not a continuous seal thus may allow bacterial leakage through the tooth. Direct pulp capping with adhesive resins on the exposed pulp has been suggested on condition that marginal micro-leakage is prevented so as to restore the tooth; trials in the monkeys and other primates reveals that adhesive systems and the composite resins are naturally compatible with pulpal tissue when correctly placed on the exposed part after bleeding is well controlled.
The level of bleeding is a sign of projection of what might happen to the capped tooth, the adhesive system after it’s used it induces pulpal responses and a varying degree of leak. The style of etching using phosphoric acid at 30% concentration is most used during the restoration process.
The current studies recommend use of adhesives instead of traditional calcium hydroxide on a direct pulp capping. Clinically put, this mode of treating is limited to the exposed pulps of less than 2mm in the diameter.
Canal therapy
When the tooth has large lesions, mechanical pulpal exposure is done and if the tooth is much broken and needs a crown then this is the time the root canal therapy is done so as to prepare the tooth for capping by making it bacteria free.
The big question remains that if the tooth canals and tiny tubes can be made bacteria free, what might happen in the spam of time; do bacteria come back and form more tubes? Indeed this is possible because it happens in the gum disease.
If it so happens, does it pose any danger? And does it respond like when the bacteria were left there during the canal treatment? According to the simple logic, the answer is yes but more research is yet to be done in this problem statement to come up with more compounded facts that help to argue out queries like these.
Hey there! My name is Dr. Moore and I specialize in General Dentistry. I have completed and found these CMEs to be very useful so I thought I’d share them with everyone.
Here’s a description of what they’re about: “Joslin Diabetes Center, through the Professional Education Department, produces continuing medical education (CME) for healthcare providers involved in all aspects of diabetes care. In line with this vision, Joslin has developed a comprehensive, longitudinal platform for Performance Improvement CME (PI CME). PI CME is becoming the accepted standard for certified medical education in the U.S., and Joslin’s PI CME platform uses a custom, turn-key approach to help you assess your practice and implement practice changes. The PI CME platform is delivered via the Joslin Professional Education Consortium (JPEC), a web resource extending traditional modes of learning with online virtual patient visits, point-of-care tools and resources, and peer-to-peer interactivity.”
In order to participate in the CMEs you’ll have to register on their website: http://www.jpec.joslin.org
If you could post this on your blog, that would be great!
Dammit!
I just typed a whole long message, and when I hit the submit button my browser freaked out.
Did it come though or do I need to redo it?